My theory is that they are not being tested because, if they were to be tested, it would throw a spotlight on Trump’s failure to roll out adequate testing across the nation. There would be a tsunami of a backlash – “the President can get a test when he needs it, but I can’t.”
Here’s a stellar article by Vox on how the whole testing deployment has been tragically bungled by the Trump Administration. It starts with a sad anecdote about a man who should have been tested weeks ago and still can’t get a test. His entire community is in jeopardy and no one has any idea if the virus has spread through it or not.
In late February, Julie Eaker, a physician’s assistant and supervisor at a small, rural, tribal community health clinic in Siskiyou County, California, had a patient who had a possible exposure to Covid-19. It wasn’t direct: They had been exposed to a person, and that person had been in direct contact with a confirmed Covid-19 case. Eaker’s patient was developing an upper respiratory infection too, and she wanted to ease their peace of mind — and protect the community — by getting them tested for Covid-19.
To this day, the patient still hasn’t been tested for the illness. And it’s not because Eaker didn’t try. The story she describes is Kafkaesque.
First, Eaker called her local health department and was told her patient didn’t qualify for testing since they hadn’t traveled to China, per the guidelines from the Centers for Disease Control and Prevention at the time. After the CDC relaxed its testing criteria, the patient was still sick, so Eaker called again. “I didn’t receive a phone call back,” she says.
The patient thought they had pneumonia and asked to be tested for peace of mind. Finally, last week, after Eaker ordered some test kits herself from a private lab, she got a call back. “The health department told me I was not allowed to use those test kits — that I ordered — without their permission!”
Eaker was horrified. So she called the CDC to confirm if the local health department was correct. “I did not get through,” she says. “I spent hours and hours and hours on hold. … So I thought I would just call the White House and talk to Vice President Pence, who is in charge of the coronavirus task force.“
She didn’t get Pence, but a White House switchboard operator told her to call the CDC.
“Somebody has got to help us,” she says, exasperated. “We’re out here on the front lines trying to take care of people.”
Meanwhile, the commercial tests the clinic ordered still haven’t arrived. And Eaker wonders if Covid-19 has been spreading in her community of 3,000 people. Siskiyou County might not have big sports arenas or universities where disease can infect masses. But it has multigenerational family homes where viruses can quickly infect a whole family, and a health clinic that’s already at capacity due to the flu.
…
Accurate testing is critical to stopping an outbreak: When one person gets a confirmed diagnosis, they can be put in isolation where they won’t spread the disease further. Then their contacts can be identified and put into quarantine so they don’t spread the virus if they’ve become infected, too. That’s particularly important for a virus like this one, which seems able to spread before people show symptoms, or when their symptoms are mild.
Ever since the first case of Covid-19 was detected in the US on January 20, the government’s blunders in creating and distributing diagnostic testing have greatly handicapped our response to the growing pandemic. Eaker’s story is not unique: Reports suggest providers everywhere are struggling to help their patients, while receiving frustrating guidance from authorities.
Dr. Anthony Fauci, the federal government’s top infectious disease scientist, called the testing situation a “failing” at a congressional hearing on Thursday.
“The idea of anybody getting it easily the way people in other countries are doing it — we’re not set up for that,” he said. “Do I think we should be? Yes. But we’re not. “
While the testing situation in America is getting better — private industry has stepped up to fill in the slow rollout of tests from the CDC, and the Cleveland Clinic announced it has developed a new rapid test that gives results in eight hours, rather than taking days — problems remain. The number of tests that can be performed per day is still limited and varies by testing facility. Part of that is due to a shortage of key chemicals needed to run the tests. It’s becoming increasingly clear that too-stringent testing guidelines early in the outbreak stymied researchers in knowing if Covid-19 was spreading in the US.
“There was clear lack of foresight,” Nathan Grubaugh, an epidemiologist at the Yale School of Public Health, says. “We were very slow to roll out testing capacity to individual places — wherever that came from, it was a very bad strategy.”
How many have been tested, how many tests are there, and how many can be tested
Part of the confusion here is that there are different figures floating around for the number of tests that have been done. As private labs take up the slack from public health facilities, there’s no centralized database of numbers.
“I think that we could have probably controlled this, if we had effective testing,” Angela Rasmussen, a Columbia University virologist, says.
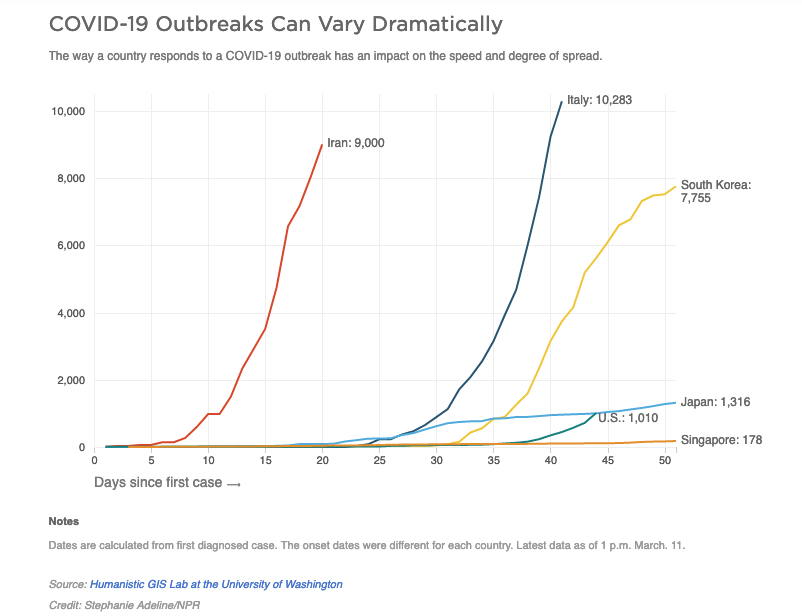
We haven’t. According to an investigation led by the Atlantic, a little more than 7,000 Covid-19 tests were performed as of early March — putting the US far behind other developed countries. (The Atlantic’s investigation was in partnership with independent researchers, and US testing counts are now being updated daily by the Covid Tracking Project.)
South Korea, for example, has tested more than 140,000 people and has even set up drive-though testing stations for people to access. So far, the Trump administration’s promises to increase testing have fallen flat.
Christina Animashaun/Vox
Test kits have been in short supply — though that’s changing.
The numbers here are a bit confusing, too. As of March 7, Food and Drug Administration Commissioner Stephen Hahn said the CDC has sent out enough test kits to test 75,000 people (far fewer than the million promised by the Trump administration). But those are just the tests sent to public health labs. An additional 1.1 million tests (produced by private industry) have been sent out to non-public commercial and academic labs, according to Hahn. In all, he estimated 850,000 Americans are able to be tested.
But capacity to test is still lagging. Part of that is due to a shortage of key chemicals needed to run the tests. Currently, according to the American Enterprise Institute, 16,030 Covid-19 tests can be processed in the US a day, up from 7,840 a few days ago. (South Korea has been able to run 10,000 tests per day since February.)
Some labs have much higher capacity than others. Even the corporate diagnostic companies like Quest and LabCorp only have the capacity to run 1,000 and 1,500 tests a day, respectively. Your ability to get tested may depend on where you live, the lab your physician uses, and the judgment of your doctor.
The timeline of the testing fiasco shows many sources of error
There’s no one reason the testing effort has been so slow. There seem to be bureaucratic, scientific, and economic drivers for the debacle.
Here’s where the trouble started. The CDC started sending out test kits to laboratories the first week of February, a month after China announced the outbreak. But the health agency quickly encountered a problem.
Some labs reported to the CDC that some of the test kits were delivering inconclusive results during verification. It’s believed that one of the chemicals used to conduct the test was not working properly and needed to be remanufactured.
…
“I’m very puzzled by what’s happened. The CDC did a really good job with H1N1 and Zika in exactly this thing: sending out huge quantities of test kits very rapidly to every state in the US and more than 100 countries around the world,” Tom Frieden, who led the CDC under President Barack Obama, told Vox. “The world came to rely on the CDC.”
…
Also, at first, the testing was bottlenecked. Most states had to send their samples to the CDC until March 2, and so, to the frustration of state health officials, precious time was lost shipping materials to Atlanta in those critical first few weeks. What’s more, each test required lengthy phone calls with the CDC, Rachel Levine, who leads the Pennsylvania health department, told Vox.
As of February 25, only 12 labs across the country — in just five states — had the ability to test. The first case of Covid-19 detected in the US originally did not meet the criteria for testing, as the New York Times explains. Perhaps that had deadly consequences: The outbreak in Washington state appears to be part of a transmission chain related to that first discovered case. When the CDC refused testing for that case, the Seattle Flu Study, a research group, performed one on its own.
Now that states can perform their own tests, they are able to turn them around in a matter of hours. “It’s a much more efficient mechanism,” Levine said, “but _it took a long time for that to happe_n.”
In Seattle, currently the US city with the most Covid-19 cases, local researchers were so exasperated by the CDC’s initial faulty test that they came up with their own, as Stat’s Helen Branswell reported:
Frustrated by the lack of testing resulting from the problem with the CDC-developed kit, the Seattle Flu Study began using an in-house developed test to look for Covid-19 in samples from people who had flu-like symptoms but who had tested negative for flu.
That testing was vital for Washington, as it led to more clues about how the disease was spreading there. Genetic detective work from Washington suggests the virus has been circulating there for at least six weeks. Modeling suggests there could be 1,110 cases of Covid-19 in the Seattle area.
So there’s been human error. But it’s also important to know that the work of setting up testing for a new virus can be difficult. Laurie Garrett, the science journalist who won a Pulitzer Prize for her reporting on the 1995 Ebola outbreak, said China’s most-used tests have had false negatives nearly half the time.
“Everybody is having trouble with the sensitivity/specificity issues” with the coronavirus, Garrett said. But the slow start to testing in America, compounded by the problematic test kits that were first sent out into the field, has set back the US response.
“I have no criticisms for the scientists at the CDC who developed the test because sometimes tests just don’t work,” Rasmussen says. But she does mention it’s problematic that the CDC has removed data about the number of people tested in the United States from its website, saying it didn’t want there to be discrepancies with state testing numbers. “In my view, the biggest scandal is that sort of response.”
Now that we have a functional test, it’s still not reaching enough people
Vice President Mike Pence and other top Trump administration officials have been promising to ramp up the country’s capacity to test for coronavirus, but they have failed to meet their goals.
As Bloomberg reported on March 5, senators were told in a CDC briefing that the Trump administration would not be ready to roll out the 1.5 million kits it had promised by the end of this week. The number would be fewer than 500,000, it appeared.
The Atlantic has provided the best accounting of how many tests have actually been conducted in the United States so far: around 7,000, according to its survey of state health officials and other sources. That puts the US far behind some of its economic peers with much smaller populations:
In South Korea, more than 66,650 people were tested within a week of its first case of community transmission, and it quickly became able to test 10,000 people a day. The United Kingdom, which has only 115 positive cases, has so far tested 18,083 people for the virus.
Making matters worse, some people who have sought tests in the past few weeks, like Eaker’s patient, have been turned away. And these shortcomings make it harder for the public health community to react to a virus that spreads quickly and easily.
Many people don’t really show symptoms of Covid-19, or their symptoms are very mild, but you want them to be tested anyway if there is an opportunity. To do that, doctors need to be able to order the test, which the CDC is only now permitting them to do. Commercial labs only recently started processing the coronavirus test, too, a step health care providers had been urging the administration to take.
“The issue is with asymptomatic transmission. You don’t know who is infected, and symptoms aren’t going to help if the patient doesn’t have any,” Abraar Karan, a Harvard physician, said. “A rapid test would help because you can then do mass testing at scale.”
Another is the criteria for who qualified to be tested. Originally, that was limited only to people who traveled to China or who had been in close contact with someone known to have Covid-19.
Then the tests expanded to include anyone who traveled to any affected country, as well as people with unexplained flu-like symptoms. Now, anyone with a physician’s authorization can be tested for Covid-19 — that is, if they can access a test.
Meanwhile, the federal government has decreased some regulatory roadblocks for more testing labs to come online. Labs can now start testing if they are pursuing an emergency authorization to test, and they don’t have to wait for the FDA to give them final approval. But some of the materials to run the tests are growing scarce for some labs, according to Stat.
What needs to happen next
We don’t need testing just to diagnose sick people coming into doctor’s offices and hospitals. We also need testing to do surveillance out in communities. “You actually have to go out now in many places in the US and start taking samples from people,” Grubaugh says.
Those surveillance studies will help us understand how prevalent milder cases are in populations. And adding those milder cases to data sets will help researchers determine more accurately how deadly this virus is, whom it tends to infect, and how often people spread it before showing symptoms. As testing ramps up, be prepared to hear about a lot more cases of Covid-19 in the US.
As former FDA Commissioner Scott Gottlieb tweeted Thursday, the private labs also need to step up. “Only big national clinical labs like LabCorp and Quest can fill the void. A lot rides on them now. … Only these big national chains have throughput, scale, and ordering systems to fill the void that was created. We look to them now. We need them.”
All that information can then be used to better halt the spread of the illness.
Again, without testing, we’re in the dark. And while we’re in the dark, the virus can spread. As Rasmussen says, “we don’t know what the prevalence actually is.”
BTW, Vox is doing an amazing job covering COVID-19. Check out their guide:
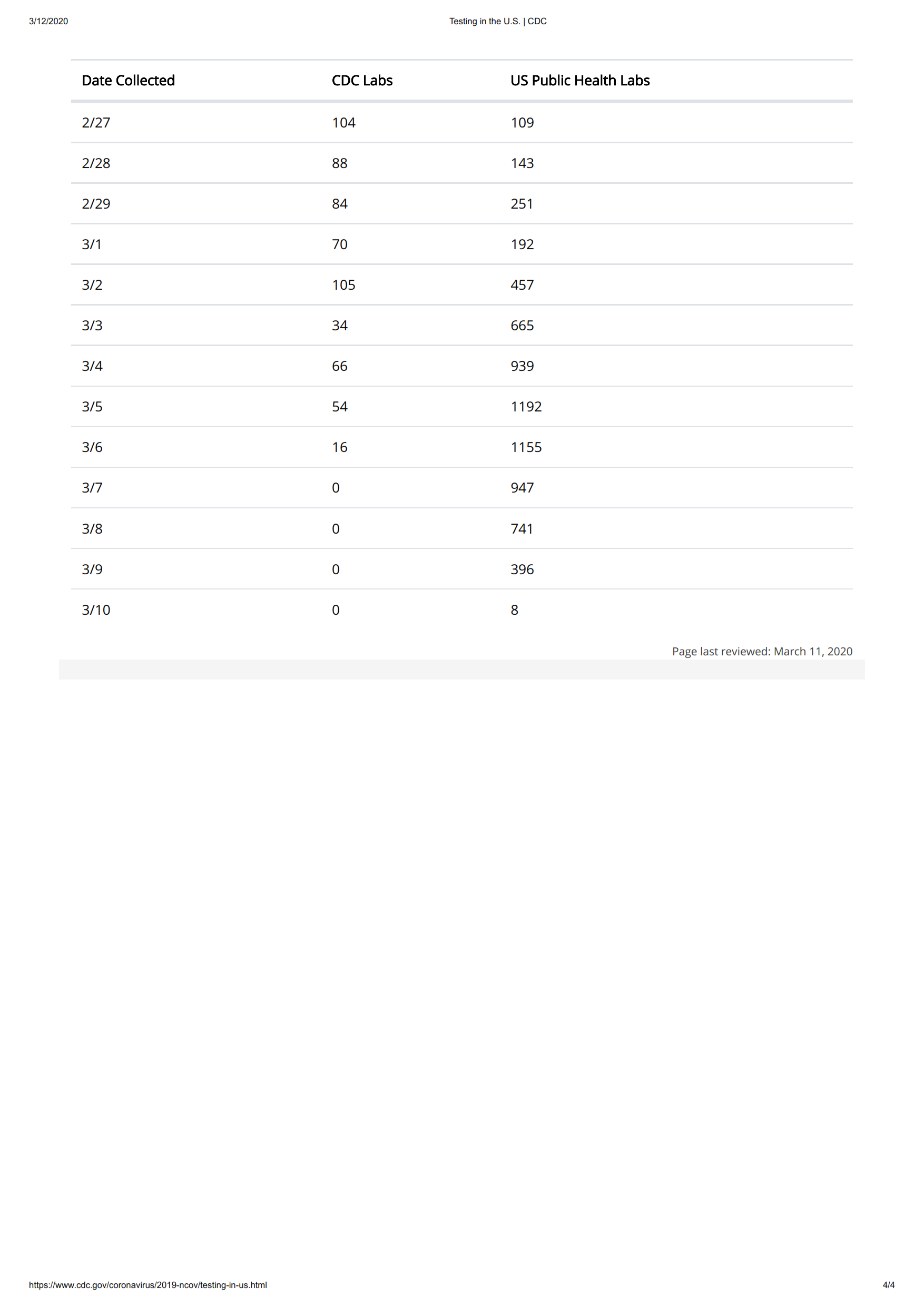
Back to the testing debacle: here’s Dr. Sanjay Gupta explaining that our government conducted only 8 tests for coronavirus on March 10. He seems at a loss for words as to why this would be. I’m thinking that private testing is now taking over as the primary testing vector, but it would be nice if the CDC would tell us this and would give us at least a rough idea of how many people are being tested – if they’re not collecting this data, they should be. Thank gosh for our diligent free press – it appears that The Atlantic is doing the CDC’s job by canvasing hospitals and clinics to put together the numbers – see the chart in the article above – it uses The Atlantic’s numbers.
I had trouble getting my head around this abysmally low number, but here it is on the CDC web site just as Gupta related (you may need to download this image and display it locally to see it clearly):



:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/19788002/covid_19_testing_per_capita.jpg)